The start of a new school year is a stressful and exciting time for both kids and parents. If you’re the parent or caregiver of a child with a bleeding disorder, you have a lot more to consider than just which school supplies to buy. There are precautions you can take before and during the year to ensure things go as smoothly and safely as possible.
Talking to Your Child
The best way to prepare for the new school year is to get together with your child, their doctor, and the school staff to agree on a plan. Start by having a one-on-one conversation with your child. Make sure they understand their condition and encourage them to speak up if they need help or are experiencing a bleed while in school. They should know how important it is to take care of their bleeds right away.
Talking to a Physician
Next, meet with your child’s hemophilia treatment center (HTC) doctor or nurse to come up with a treatment plan. Talk about your child’s participation in sports and other physical activities. You should sit down with the HTC doctor or nurse before any meetings you have with the school regarding bleeding disorders, because it is good to have an overall understanding of things yourself.
Talking to the School Staff
It is important to plan a meeting with the school staff before the school year is in full swing. If you haven’t done this yet, try to organize a meeting as soon as you can; don’t wait for back-to-school night when teachers will be busy meeting with many parents in one evening.
Contact the school nurse, counselor, or principal to organize the meeting. You should talk about safety precautions, the storage and possible use of treatment in school, and the importance of not singling out or embarrassing your child. People who should be at the meeting include:
You and your child
Primary teacher(s)
Gym teacher
School nurse
An administrator (eg, principal, vice principal)
A previous teacher who has experience with your child’s condition (if available)
What to Do During the Year
During the school year, your child needs to be comfortable speaking up if or when bleeds occur, and teachers should be able to recognize bleed symptoms as well. Provide them with a checklist of basic symptoms, as well as an emergency contact list of whom to call if a bleed happens. The same goes for gym class and after school activities—if your child can participate in these activities, the staff should be on the lookout for bleeds or other issues.
If the bleeding disorder causes absences or missed schoolwork, you, your child, and their teacher(s) should work together to figure out the best way to get caught up. Your child should know that it is okay if their condition prevents them from completing some work on time, but that bleeds are not an excuse to put off responsibilities.
Working as a Team
Perhaps the most important thing is to keep in mind that everyone involved is part of a team. You all have the same end goal: to help your child have a productive and enjoyable school year. The school staff may not have much experience with bleeding disorders, which is why it’s important that you all work together throughout the year to ensure your goals are reached.
For printouts on bleed symptoms, emergency contact information, and other useful resources for the school and your child, visit the NovoSecure™ downloads page.
We’ve
been focusing on changing therapies in the hemophilia community the past two
years, including products that give us more options and choices. Read below to
learn about how Biogen scientists developed two products that are being used to
help improve hemophilia care.
Please see below for the Indications
and Important Safety Information
In
2000, Rob Peters and Jenny Dumont, currently top scientists at Biogen, wanted
to make a difference in hemophilia care. They saw that hemophilia therapy
hadn’t changed since the 1970s and there was an unmet need for a
new class of treatment.
Rob,
Jenny, and their team knew it wouldn’t be easy. They were fully aware that it
often takes years, even decades, to get a therapy from that spark of
inspiration through research, clinical trials, and FDA approval to the
community who so eagerly wanted an alternative therapy.
Rob
has a PhD in biochemistry from Harvard and is a VP, Hematology Research, at
Biogen. Jenny has her PhD in cell biology from the University of Cincinnati
College of Medicine and is the Medical/Scientific Director, Global Medical, at
Biogen. Both certainly had the education and training to tackle such a daunting
challenge. More importantly, Rob and Jenny had an unwavering passion to develop
new therapies.
Their
passion helped them stick with it and in 2014, after a decade and a half of
hard work and determination, Biogen launched prolonged half-life ELOCTATE® [Antihemophilic
Factor (Recombinant), Fc Fusion Protein] and ALPROLIX®
[Coagulation
Factor IX (Recombinant), Fc Fusion Protein].
Prolonged
half-life ELOCTATE and ALPROLIX have been helping people with hemophilia for
the past two years. In that time, doctors have written thousands of
prescriptions.
Rob
and Jenny recently returned from the National Hemophilia Foundation and World
Federation of Hemophilia meetings, where they had the opportunity to talk with
people who have been taking ELOCTATE and ALPROLIX. They got to see, firsthand,
that their perseverance and passion was well worth the effort.
“Bringing
ELOCTATE and ALPROLIX from inception to the people who need them was a lot like
raising children,” Jenny says. Jenny is a mother of 2 and grandmother of 3. “You
give them so much of your energy and attention for so many years, then let them
go into the world and hope they make an impact.”
Rob, father of eight-and-a-half-year-old twins, agrees, adding: “I was raising my twins the
same time we were developing ELOCTATE/ALPROLIX. That really helped me
appreciate the potential of what more time between infusions could mean in the
lives of families with kids with hemophilia.”
ELOCTATE
is an injectable medicine that is used to help control and prevent bleeding in
people with hemophilia A (congenital Factor VIII deficiency). Your healthcare
provider may give you ELOCTATE when you have surgery.
ELOCTATE Selected Important Safety
Information
Do
not use ELOCTATE if you have had an allergic reaction to it in the past.
ALPROLIX
is an injectable medicine that is used to help control and prevent bleeding in
people with hemophilia B. Hemophilia B is also called congenital Factor IX
deficiency.
Your
healthcare provider may give you ALPROLIX when you have surgery.
ALPROLIX Selected Important Safety
Information
Do
not use ALPROLIX if you are allergic to ALPROLIX or any of the other
ingredients in ALPROLIX.
There’s been a lot
of change in our community this year, but perhaps none so impactful as the
change in Baxalta, now a part of Shire. Please read below to learn more about
these changes, and click through to learn how Shire will keep on serving you!
Shire, is built on
strength and experience, and is powered by an enduring commitment to you. Each
company brings world-class products, as well as, a foundation for sustained
category leadership in rare diseases.
Combining 60 years
with 30 years of dedicated history to bleeding and rare disorders communities,
the new company has even more resources to offer. What that means for patients
is that Shire is maintaining its solid commitment to you while still offering
innovative products. Introducing new treatments for bleeding disorders, and
making a meaningful difference in the lives of patients and families continues
to be Shire’s main focus.
Shire’s combined
product offerings have expanded the range of therapeutic areas. Shire and
Baxalta are combining 30 years with 60 years of dedicated history to the rare
disease and hematology community. Together they are commitment to the
hematology community.
The true result of endeavor, whether on a mountain or in any other context, may be found rather in its lasting effects than in the few moments during which a summit is trampled by mountain boots. The real measure is the success or failure of the climber to triumph, not over a lifeless mountain, but over himself: the true value of the enterprise lies in the example to others of human motive and human conduct.” —Sir John Hunt, leader of the 1953 British expedition that first ascended Mount Everest
Ready to roll! Kilimanjaro: the CEO Challenge 2016!
This was a week of triumph over self, as our group of nine attempted to summit Kilimanjaro, the largest free-standing mountain in the world and the rooftop of Africa. Kilimanjaro was born 300 million years ago in fire, when massive tectonic plates in Asia shifted, creating the Great Rift Valley and pushing up sections of the earth that eventually formed the volcano Kilimanjaro. If you climb Kili, like I did this past week, you will see miles of enormous lava rocks of black basalt littering the mountain, rocks that were birthed deep in the womb of planet Earth and blasted out when the volcano exploded. During the ice age, glaciers formed, adorning sections of Kili with massive frozen sculptures.
I thought of the similarities to hemophilia this week: bleeding into joints is the fire, the pain; ice, the pain reliever. And trying to improve hemophilia health care in developing countries? A grueling climb up a mountain is a good metaphor. For a successful climb you need self-discipline to get in shape, leadership, guides or a map, a compass, equipment, trust in your guide, and trust in your teammates.
Our team? An amazing group! Eric Hill, vice president and COO of Diplomat Specialty Infusion Group, and his 15-year-old son Andrew. Eric serves on our board of directors for Save One Life and sponsors 31 children. Eric climbed with me in 2011 with his son Alex. Rich Gaton, co-founder and president of BDI Pharma, a specialty distributor that provide hemophilia and other therapies. Rich’s company is a proud member of Save One Life’s Dedication Circle, sponsoring 20 beneficiaries over the past eight years. With Rich are his wife Wendy and two daughters, Taylor (20) and Samantha (16). Mike Adelman, vice president of commercial operations for Aptevo Therapeutics, Inc., manufacturers of the recombinant factor IX product Ixinity. And Jim Palmer, MD, a surgeon from Philadelphia and friend of Mike’s. Individually, we wished to triumph over self. Together, we climbed to raise over $65,000 for Save One Life.
Day 1: August 7, 2016 Sunday
We all gathered in the lobby of the Kibo Palace hotel in Arusha, Tanzania, excitement shocking us like static electricity each time we hugged one another good morning. Our guides, Hesbon, Kelvin, Victor and Edwin, helped us put our stuffed rucksacks on the bus. We clambered aboard and squeezed in among porters, guides and bags. It was a two-hour ride to the Machame Gate, where our adventure awaited.
First we stopped at the familiar store we stopped at five years ago, when Eric and I and another group summited Kili, to pick up snacks. We sat about in the sunshine on the grass, waiting for the guides to return. Hesbon went with me across the street to a shop to get a Nalgene bottle, for $7 which he fronted. I don’t think I ever even used the bottle in the end.
Finally, back on the road. We passed roadside shops and rural homes, dust swirling from our speed. When we reached the Machame Gate (elevation 5,718 feet), we felt pretty calm. Outside the gate, a mob of vendors hawking shirts and hiking supplies. Inside, the gate was swarming with hikers, porters, bags. It would be a very late 12 pm before we started our official hike. In the meantime, Hesbon filled out paperwork while we put on gaiters and filled our Camelbacks with water. We would carry a 25-lb daypack each day while our porters would carry our 50-lb rucksack, along with their own daypack and all the accouterments of camping for nine: mess tent, folding chairs, port-a-potty, our tents and mats, and food for 29 porters, four guides, a cook and nine hikers for six days!
Our first day then had us hiking about six hours to the Machame Camp, elevation 9,927 feet. The route was a groomed trail for the most part, through a dense and moist rain forest. It was cool and progressively dark. The forest was lovely, lush green, with trees covered in soft moss, making them resemble a young deer’s antlers, covered in velvet. Many birds serenaded me. One had a distinct sound: “Tweet… bong!”
Hitting the trail!
The hike was harder than the team expected and harder than I recalled from five years ago. Very steep, working our quads and calves intensely. At times we broke away from one another, then paired up with different teammates. Wendy took her time as she had asthma; husband Rich stayed by her side the entire day. The lead guide Hesbon also needed to stay with her as he always would be last to enter camp, to ensure his hikers were all present. Mike was stricken with food poisoning the night before. The hike was very difficult for him but incredibly he persisted and arrived at camp one. By 6 pm, the weather turned rainy and cold as we all stumbled at various times into camp. It was dark. Camp was crowded with people, so different than five years ago when there were perhaps three teams, spread out comfortably over the camp ground. Now there were maybe ten teams, with all their gear and porters and tents. Pandemonium in the dark, as we all shivered in the rain, waiting for our team to assemble and find one another! Our porters had our camp ready, and we finally found our tents and crawled inside.
I had a single tent; everyone else shared one. As I would each night, I laid out my sleeping bag, stuffing in my clothes for the next day to keep them warm when I awoke and placed necessary items for the night close by: Kleenex, water, cough drops. I was nursing a cold that would later strike my chest and make the hike difficult for me. One by one, we were being hit with physical challenges to the climb. Dinner was welcome, though we had to grope our way in the dark to the mess tent, careful not to trip on the tent stakes. Juju, a young man who doubled as a porter, would serve us each night. Each dinner usually started with steaming soup, rolls, followed by a main course– chicken, rice, beans, for example. Our team sat about the table, eating, joking and comparing experiences of the day. By 9 pm we went back to our tents, and crawled into our sleeping bags.
Day 2: August 8, 2016 Monday
Gaton girls at the Shira Cave Camp
I awoke at 4 am to the sounds of the porters preparing for the long day ahead. I had a pretty good night’s sleep though. My sleeping bag, rated for 0°, is toasty warm, making it hard to leave each morning as the temperature dropped more and more the higher we went. Each day started the same: Juju and Able brought us each tea or coffee first thing, to warm us up in our tent. This was a luxury, tea in “bed”! Then, they brought a plastic bowl filled with very hot water, to wash and brush our teeth in. You cannot imagine how important one little bowl of water becomes. Kilimanjaro is very dusty, and even by day two we were coated in dust. Washing was a luxury, and that little bowl of water became something I was excited to see each morning.
Breakfast on Kili
Then breakfast: usually a round of fried eggs, toast, jam, more tea or coffee, pancakes. Yes, they prepare all that fresh for us each morning! We top off the Camelbacks with water, toss in electrolyte pills, stuff in our rain gear (you can’t go anywhere on KIli with rain gear) and anything else needed for the day, pack our sleeping bags and clothes in the rucksack, and get ready to leave.
“Twende!” shouts the guide Kelvin, a big guy, at least 6 feet tall, who walks with a noticeable limp. Let’s go! We had our concerns about his limp, but also learn he was a national soccer player in his time. The leg injury forced him to retire, and he was able to still climb well, despite it. Mike is still not well, Wendy was much improved overnight, and the Gaton girls each have slight headaches, from the altitude. We are all taking Diamox, a hypertension drug that doubles as an altitude-sickness pill, but symptoms still appear in each of us from time to time.
Laurie Kelley and Mike Adelman hit the trail on Day 2
Today’s climb was through a completely different geological zone, the Moorlands. Gone were the towering green trees and milder temperatures of the rain forest. Starting our hike with a bang, we immediately ascend a rocky path that leaves us gasping. The entire day would be spent climbing on rocks and not a trail, much like my Mt. Washington training hikes. The air was cold, and we were encased in cloud cover all day. We would miss some stunning views of nearby volcanoes, as we could see little but the path ahead. As we ascended, we put some space in between us on the hillside; through the mist, seeing other climbing parties in their various colored rain gear, I thought we looked like brightly colored beads strung on a necklace draped on the grey neck of some ancient beast.
We passed the hardier vegetation in this cold climate: the Everlast plant with its pretty flowers, and the “antifreeze” plant, which closes each night to protect itself from the cold. The topography has changed radically.
We climbed from 8 am until 2 pm, reaching Shira Cave Camp, at 12,355 feet. By now everyone was feeling good, except Mike. But he never complained, and still kept plowing forward on this difficult hike. At 4 pm, Edwin, a cheerful 28-year-old guide, asked us if we wanted to do a 45-minute acclimatizing climb while dinner was prepared. Despite the large number of climbing parties, there was more space at this camp, and we spread out. Eric, Rich, Mike and I all did the acclimatization climb, which was not hard. I felt great at this altitude and relished the climb on the rocks, which were beautiful.
Jim Palmer, our team doctor and new friend!
Later in my tent, I wrote a bit about the day and felt the cold seeping in. Tomorrow will probably be freezing temperatures when we awake!
Eric Hill and son Andrew: my second time climbing Kili with Eric!
Day 3: August 9, 2016 Tuesday
Our strong porters
I wondered when I woke up, why am I doing this? Sleeping in a bag on the ground, freezing cold, facing a long hike ahead. I could be home, clean and warm, having summer fun! That was the one and only time I thought this during the six days, caving in for a moment to a human desire to escape misery. Instead, I switched to thinking what fun this was, to challenge oneself, to share hardship with fellow teammates, to see who and what we all are deep inside. I dressed careful within my sleeping bag, then braced for the cold. Frost etched all the tents as we emerged like lethargic bears awakening from hibernation. The sky had cleared! Now we could see other volcanoes, including the summit cone of Kilimanjaro, Kibo Peak. That was our goal! Everyone was excited. Our goal! Kibo Summit on Kilimanjaro Still smiling!
Our goal! Kibo Summit on KilimanjaroStill smiling!Lava Tower
By now I was coughing with a chest cold, complicated by all the dust and increasing cold air. Everyone else was well but coughing too. This would continue for days even after our climb. Breakfast was high energy and we could feel anxiety; we wanted to get going. Breakfast was hot but soupy porridge, toast and tea, and fried eggs. By 7:30 am we were on the trail, looking forward to a four hour hike through the Barranco Valley. This was a totally different kind of hike today, mostly flat with a few hills to navigate. Victor, our guide, took my camera and snapped dozens of photo of us as we climbed. We had on warm outerwear now, as the wind picked up. By noon we were at the Lava Tower, a massive rock formation jutting out of the ground, looking a lot like a mini version of Devil’s Tower in Wyoming. Perfect spot for lunch and we all joyfully sat at the table. By now our team had gelled beautifully with each person playing a role. Mike was our jokester, keeping everyone laughing with his witty remarks. Samantha was our musician, and she and Mike began thinking of songs we could sing to use pole pole, which means slow, slow in Swahili. It was hysterical listening to the many songs of the 60s and 70s that accommodated this but my favorite was set to Mony Mony.
Descending into Barranco Valley
After lunch we checked gear, loaded up our stuff, and headed out for one of my favorite parts of the climb: the descent into the Barranco Valley. Our plan was to ascend all morning, to 15,000 feet, which we did at Lava Tower, then descend and sleep at a lower elevation, so we can acclimatize better. Barranco Camp, our goal, was at 13,066 feet. Passing through a natural gate of volcanic rock, we descended into the valley carefully. The topography changed again, with rocks surrounding us on the hills, and strange trees appearing, designed to withstand the wind and cold. These giant senecios are actually cousins to the daisies! And they looked like truffula trees, whimsical creations of Dr. Seuss, which was appropriate as each black boulder we passed was coated with moss, that appeared as little yellow fu manchus. It looked comically like hundreds of black-faced Loraxes were watching us pass through the truffula tree forest!
Strange senecio trees
As beautiful as the descent was into the valley, the cold was seeping into our bones. Even Rich Gaton, who is so stoic and strong, confided he was freezing. My chest cold was painful and persistent now, and my nose was running chronically. When we arrived at camp, dotted about with colorful nylon tents, the weather was foggy, dreary, and cold—so cold. How would we do the summit if this bothered us? Andrew and I were shaking in our rain gear while heading for dinner at the mess tent. Our tents for sleeping that night were close together, so much that when Wendy or Rich so much as rolled over, I would know it! I felt badly as my coughing was going to bother my teammates. Wendy always seemed to have the right medicine for the right moment. She was our warm nurturer on the trip, despite struggling with asthma in the cold air this entire time.
Day 4: August 10, 2016 Wednesday
Summit Night!
We must embrace pain and burn it as fuel for our journey.—Miyazawa Kenji
Mike demonstrates how cold it is!
Today we would climb to 15,239 feet to Barafu Camp, the final camp before the summit assault. First we faced a 7-hour hike, including scaling an 800-foot rock wall right after breakfast, then a long hike to camp, braving cold but more detrimentally, dust. We were excited, though! We started our day with the usual hot tea in the tent, followed by my priceless little blue plastic bowl of hot water. By now we have given up any semblance of being clean. Dust is everywhere. Breakfast is a time to share, be social, joke, check in with one another. Everyone was doing well, with an occasional high-altitude headache that faded after ibuprofen doses.
We geared up, and began the climb. Again, one of my favorite parts of the trip! My quads are feeling fantastic after all the training I did this summer, hiking Mt. Washington and working with my trainer, Dan French. In fact, I would not use my trekking poles on the entire journey, except for the rapid descent after the summit. So here, I vaulted straight up the wall using my quads and balance. Everyone did well; everyone scaled it and enjoyed photos at the top, where a crystal blue sky greeted us. The view—spectacular. We could see down into the valley. Our camp was now just a colorful speck. Our team was smiling and happy!
Onward with no time to lose. We marched down the valley, on slippery, dusty trails that plummeted down at 45° angles at times, maybe even steeper. Our guides held our hands and prevented falls whenever possible. At the bottom, we crossed creeks, jumped rocks, and made it to a flatter surface, dusty with volcanic ash powder, and dotted only occasionally by the oddly placed massive boulder. It was a surreal, primitive, prehistoric landscape. Grey and black base, domed by a brilliant blue ceiling. We were feeling the effects of altitude, which slowed us a bit. Eventually we started to ascend again, up the trails, where flat slabs of shale chimed when we stepped on them, adding a touch of class to the barren landscape.
By the time we reached base camp, we were struggling with oxygen, sunburned and elated! This was it. What we came for. What we prepared all year for. The Moment! The entire camp was perched on a mountainside, and before us was the stunning, magnificent Kibo Peak, beckoning us to climb. We could clearly see its white glazed top, its rocky sides. Kili is a beauty of a mountain. I felt awed and honored to be standing before it. I made my way to my tent, ditched my backpack and gear and wandered about till all of our team made it to the camp. My coughing had gotten worse and my voice was hoarse and raspy. Hesbon offered antibiotics as a precaution. My lungs are my Achilles Heel, so I took them. They immediately gave me severe heartburn, so badly I was not able to eat much lunch. This was a bad sign as I would need my energy to summit.
But attitude and motivation go a long way, and I was pumped up! Our plan, explained Hesbon to the group, was to have a light dinner, then return to our sleeping bags to catch maybe a few hours of sleep. Then we would depart in two groups: the first was Eric Hill and son Andrew, who proved to be the mountaineers of the group. They could go faster than us and wanted to not have to stop for breaks (stopping for frequent breaks can refuel the climbers but can also allow the cold to settle in, and can actually demoralize the faster climbers who crave to keep moving). Their guide would be Kelvin, and they’d leave at 1 am Thursday morning. Our group was the second group, guided by Victor, including everyone else. We’d leave at midnight. Wendy opted not to summit, which was disappointing to all, but the right decision. She had struggled with asthma and dust the entire day, and it was quite frankly astonishing she was even at base camp. As sweet as she is, the woman has a core of steel!
I actually was able to get some sleep, though had to pass on dinner, as my stomach burned with the aftereffects of the antibiotics. At 10 pm, I awoke and started planning what to wear to the summit: layers. Incredibly, the weather was mild, at only 20°, with almost no wind. This was a stark contrast to five years ago when it was -5° with 50 mph gusts, freezing us, sapping us of strength, and cloaking any view with white out conditions. We couldn’t get off Kibo fast enough then. This time would be radically different.
We gathered in the mess tent and did a gear check. We were each assigned someone to carry our backpack and monitor us. Team Kilimanjaro does a great job of motivating climbers as well as monitoring their physical condition for signs or mountain sickness. Off we went!
The guides forced us to go pole pole. One step, then another, as slow as possible. They also created a rhythm, so important in keeping your pace and momentum. The night was clear and millions of stars burned overhead. It was a night created for a perfect summit! Step, swing, step, swing went our gait. Up, up the rocky path to the summit. I monitored the time and by 1:30 am we had our first break. Hydrating is key, though water tends to freeze in the Camelback tube. I looked upwards at the infinite sky and saw constellations: Orion the Hunter, Taurus, and then Cassiopeia, shaped like a W. The W was upside down, forming an M (for mountain?) over Kibo, and it guided me through the night. Twice I saw shooting stars, like fireworks celebrating our summit. I took the time to take out my iPod and started playing music to keep me going. Five years ago I lost track entirely of the night, and 7 hours merged into memories of only about an hour. Not this time: I played about three hours of Metallica and the Doors, and then Guns N’ Roses. At 5 am, I was actually dancing with the porters on the mountain, gyrating as they sang, then playing air guitar to Welcome to the Jungle….
Our goalClowning around at base camp: 15,000+ feet!
And then the iPod died. I knew from then on it would be a struggle. While hoping to summit at 7, our group was slow. This was good as no one got sick, but it depleted that much more energy. The guides forced Red Bull down us, which I detest but drank. It instantly gave us energy. Stinger waffle snacks, Gu gel, hot tea, anything to keep us energized. But the energy drained away. I bonked. I had been running on music and fumes and now my music was gone. It did a psychological number on me. Why didn’t I keep a second iPod in my other pocket! (Note to self for next time…)
I thought about the kids I know who struggle with hemophilia and poverty. This suffering was ordinary, a luxury, self-imposed. No big deal. Just put one foot in front of the other. The trouble was, my feet would not always respond to my commands! Victor took my arm and guided me, assuring I would not stop or sit. Sitting down was the kiss of death on the summit climb and was not permitted.
Mike was now doing great, finally over his food poisoning and feeling strong. Amazing! Jim was confidently plugging away, and never once seemed to fatigue. Rich Gaton and I climbed closely together, with his daughters. Without their mom there, I felt a deep need to stay close to the girls. They are strong, but I had done this climb before and knew the pitfalls. Self-doubt, giving in to fatigue, wanting to quit—been there, done that. Rich and I conversed, which was nice, as it kept our minds off the fatigue. Dawn broke behind us, a red orb peaking through the clouds below us. Funny, sunrise was happening below us! Above us, the summit.
Day 5: August 11, 2016 Summit Day!
Incredibly, we reached Stella point at the brilliant dawn of day, at 18, 848 feet. This was a milestone for sure, and you could see Uhuru Point, at 19,349 feet, the official summit, up ahead. It seemed so close and, in my mind, addled by lack of oxygen, I thought it was only a ten minute walk. I told this to Taylor, who was exhausted and ever so politely said, “I think I’ll stay here at Stella,” and sank to a rock. We cajoled her, and I told her just ten more minutes! Think of how you will feel if you stop now! Hesbon pulled her up and she stumbled on. I needed Victor too to guide me on. The ten minutes was actually another hour! Perhaps the hardest hour of the entire six days was getting from Stella to Uhuru, but we all did it.
We did it! At Uhuru Peak, the summit! Save One Life team
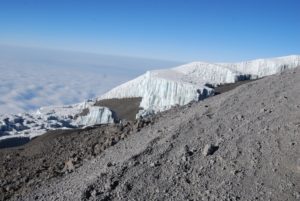
We hugged, we posed for photos with our Save One Life banner, and actually explained to some fellow summiters what the program was all about. I looked about at the view I couldn’t see five years ago when I first summited. There are no words: a massive volcano, with a deep caldera of lifeless moondust, shocked with gargantuan glaciers. The glaciers are blue tinted rectangular structures that you could compare to alien spaceships, or modern architectural skyscrapers or, as Taylor put it, like the rocket popsicles we ate as kids. I struggled to find a way to describe their icy beauty, like frozen fortresses on display for millions of years.
We needed to get down as oxygen is only 50% at the summit. We linked up one by one: Jim, Mike, Rich, Samantha, Taylor, me, our guides, and started the descent. Eric and Andrew were already on their way down. This would take over 5 hours and was another punishing trip. But for now, we gleefully focused on the goal we achieved and worked so hard for: the summit. Somewhere in my oxygen-deprived head, I was also thinking of what this could mean for Save One Life and the patients we serve. Money for programs; motivation to keep persevering despite setbacks and challenges; and perhaps, another summit climb, when more captains of industry like Rich, Eric and Mike join us to experience the outer limits of endurance, to raise money and awareness for hemophilia in developing countries, and to triumph, personally and professionally. When there is a common cause to help others who suffer, a purpose bigger than ourselves there seems to be no limits to what a group of compassionate people can accomplish.
Thanks to my teammates—you are strong, exceptional, compassionate and brave! In particular, thanks to Eric Hill for suggesting this climb and for his leadership, and to Dr. Jim Palmer for his advice, services and wonderful attitude! Thanks to Team Kilimanjaro for safely escorting us on this amazing journey. Thanks to everyone who contributed to our fundraiser, for you made this climb successful and worthwhile. Please visit Save One Life to learn more about how to sponsor a child with hemophilia in need, or to get involved. Get ready for the Kilimanjaro CEO Challenge… 2017?
Disease and disasters come and go like rain,
but health is like the sun that illuminates the entire village. Kenyan proverb
I’m back in Africa where, contrary to popular
belief, it is not scorching hot but cool and pleasant, lush and green. It’s
winter here, and the mornings are moist and overcast, later clearing to blue
skies and mild temperatures. I’m in Kenya, in particular, visiting the children
and young men who participate in Save One Life, our child sponsorship program. We
work through our in-country program partner, The Jose Memorial Haemophilia
Society, established ten years ago by Maureen Miruka, mother of a child with
hemophilia. They’ve been fantastic to work with and this is my fourth or fifth
visit to Kenya, a country I’ve come to love. Over just two days we will visit
six families around the capital, Nairobi, and in Murang’a, a town about 90
minutes away from Nairobi.
Our volunteer US team arrived with multiple heavy
bags, packed with gifts for the families (t-shirts, caps, toys, candy, school
supplies) and our hiking gear, for following this trip we will climb Mt.
Kilimanjaro as a fundraiser for Save One Life. In fact, as this is posted
automatically on Sunday, I have already started my climb by now!
After our first Kilimanjaro climb in 2011, we
raised $65,000 for Save One Life, for our Africa programs. Many people in our US
and global community asked if there would be another climb. Particularly, some
executives from industry wanted to climb, so we arranged a “CEO Challenge,” for
those captains of industry to not only climb, not only raise money for Save One
Life, but to experience a world vastly different from their own firsthand, at
ground zero. To experience, even for a day or two, the lives of the poor with
hemophilia in a developing country.
Save One Life’s volunteer team with JMHS at
Stanley’s home
Our volunteers from the US are Eric Hill, vice
president and COO of Diplomat Specialty Infusion Group, formerly vice president
of BioRx, and his 15-year-old son Andrew. Eric serves on our board of directors
as treasurer and has been invaluable for his expertise and dedication. He
sponsors 31 children! Eric climbed with me in 2011 with his son Alex. Eric and
I know exactly what kind of suffering we are in for! We also have Rich Gaton,
co-founder and president of BDI Pharma, a specialty distributor that provide
hemophilia and other therapies since 1995. Rich’s company is a proud member of
Save One Life’s Dedication Circle, sponsoring 20 beneficiaries over the past
eight years. With Rich are his wife Wendy and two daughters, Taylor (20) and
Samantha (16).
Sarah Mumbi of the JMHS
Also with us are Mike Adelman, vice president of
commercial operations for Aptevo Therapeutics, Inc., a new company spun out of
Emergent BioSolutions, manufacturers of the recombinant factor IX product
Ixinity. Joining us on the Kili climb is Jim Palmer, MD, a surgeon from
Philadelphia and friend of Mike’s, who is also
fundraising for us!
Our day Thursday started off with a hotel pickup
by Maureen Miruka, our long-time colleague, founder and president of the Jose
Memorial Haemophilia Society, dedicated in memory of a son she lost to
hemophilia. The JMHS is our program partner in Kenya, and through it we sponsor
47 children and adults with hemophilia, with two more registered and waiting to
be sponsored. With her were Sarah, the office administrator, a quiet and lovely
recent college graduate, with beautiful eyes and cascading braids. Maureen
whispered to me, “Sarah is a godsend. She is efficient, responsive and
intelligent. I want to keep her on!” And the charming, energetic and gregarious
Kehio Chege, father of a child with hemophilia, and board member of the JMHS.
Maureen Miruka, president of JMHS,
Jane Mugacha, pediatric nurse and Sarah Mumbi of JMHS
We loaded up the two safari style vans with gift
bags, our cameras and water, greeted our “pilots” (drivers) with a quick jambo (hello), hopped in and drove off.
Navigating the Nairobi traffic, we had time to chat about our mission and
hemophilia in Kenya. Maureen provided background on herself to the group, how
she founded her society, and plans for the future.
At this time, Kenya does not provide factor for
its estimated 3,000 patients. Treatment is centralized at the Kenyatta
Hospital, the large public hospital in Nairobi. Project SHARE, operating from
my company, LA Kelley Communications, has provided factor for Kenya over the
past 15 years, as has the World Federation of Hemophilia. We continue to
provide factor to both the JMHS and the Kenyatta National Hospital. Of the estimated 3,000 with
hemophilia in this country of 44,000, only about 500 have been registered. Of
the 500, only about 150 are “regulars,” that is, we know who they are and where
they live. The others are what I call transient patients: they may have visited
the hospital once in their lifetimes, or have visited a few times, but not
regularly. In developing countries, people move about frequently, sometimes
living with relatives in different towns, villages or addresses in the cities,
as they struggle to make ends meet.
And most of the hemophilia patients here are
poor. These are the ones enrolled in Save One Life, a few of which we would
visit today.
We zoomed past roadside markets, bursting with
fresh fruits like papaya, watermelon and bananas, managed by women in colorful
clothing. City fell away to countryside in no time. The tall buildings and
billboards of Nairobi transformed into banana trees, tea plantations and
rolling hills. Kenya is beautiful, like so much of Africa. The climate and
topography, the images and animals all have captured the attention, dreams and
affections of visitors.
Our first stop after a 90-minute jaunt was the
Murang’a District Hospital, to meet with the hospital chief, tour the wards and
offer a gift of factor. Jane Mugacha, nurse and our main contact there, showed
us the pediatrics ward (“My home,” she said, holding her hand to her heart),
where a small refrigerator held a few vials of factor. “This is where the
patients come to get infused locally,” she shared. Murang’a is 90 minutes from
Nairobi and so it is far better to store factor here. This sounds
logical, but trust me, in developing countries most hospitals have no
factor except the main government ones in the capitals. Patients have to travel
hours, sometimes days, to get treatment for bleeds that by then have already
done their damage.
Wendy Gaton with Stanley
I’m sure Rich and Eric were shocked at how little
factor was stored, when back home, their inventories were chock full for the
insatiable American hemophilia market. We donated about 30,000 units, more than
tripling her current stores. Jane was ecstatic, effusive in her praise, for
just this small amount!
I pointed out to Wendy and her daughters the
“waiting room,” of the hospital: wooden benches outside under a steel-corrugated
roof, overlooking an unpaved, red dirt parking lot. And people wait and wait;
the hospital is always busy, always crowded.
Stanley’s farm
We chatted outside, then said kwaheri, and left to see patients. About
15 minutes away we arrived at Stanley’s home. I last visited Stanley in 2011,
and he was in a new packed-mud home now, on his mother’s property. Stanley has
hemophilia, is rail thin, and rather somber at first. (This would all change
after an afternoon spent with Kehio and our guys.) We hiked down a dirt path
bordered with sprouting vegetation, leaving the drivers and our safari jeeps on
the road. Everything is red—the dirt, the mud structures— and green—the tall
grass, the banana plants, the papaya trees. Beyond the rusty colored home were home-made
wooden pens for farm animals: two mud-covered cows for milk, a few goats, and some
chickens. Stanley looked good since the last time I had seen him, walking, even
though his gait is a bit hobbled. This was my third visit to his home. Since
that time a new child had been born, a boy, who was now almost five. He stared
at our group with wide eyes.
Stanley
Stanley is too old to be sponsored (and looks
even older than his years), but he was the recipient of a micro-enterprise
grant. Stanley shared how farming took a huge toll on his joints and caused
bleeds. He had to hoe, hack, pick and carry crops to be sold at the markets.
It’s backbreaking work for someone with hemophilia. Save One Life had given him
a grant to start a shoe vendor business, selling shoes at the market instead.
It didn’t work out as he had hoped, and with the money left he instead bought a
cow. He now sells milk daily to a local school. He earns only about $50 a
month. We visited the cows in their pen, and Maureen, who has a PhD in Agricultural Research and Development and also is Director of Agriculture and Markets for CARE USA,
questioned Stanley on the condition of the cows. Their hip bones and ribs jutted
from their paper-thin skin. Dried mud dotted the flanks of one cow, and her
hooves stood deep in feces. Behind her, bordering the woods, a mountain of
manure. All very unsanitary.
Our main question that day: what do you need?
Stanley didn’t hesitate: concrete, to build a safe and slanted platform for the
cow to stand, to separate her from the manure, and to make it easy to wash off
the manure and mud. Rich Gaton, ever the man of action, asked how much and
when? I love it! We could make an immediate and concrete difference, no pun
intended, in Stanley’s life today. It’s what Save One Life is all about.
Maureen and Stanley chatted about the logistics,
and Maureen promised to get back to us with an estimate for building a concrete
platform. Samantha and Taylor, cow lovers like me, wanted vitamins as well for
the cows. At the very least, a vet should look in on them.
Derrick
Our next visit was to see Derrick Chege, and
Stanley accompanied us. When Eric, Maureen and I last saw Derrick, he was two,
and had an enormous, disfiguring hematoma on his forehead. We thought it was
only a hematoma, but Maureen told us this day we were wrong; it was a
psuedotumor. Pseudotumors are not seen in the US for hemophilia. They are pulpy
masses of blood created from repeated, untreated bleeds into one area. Blood
vessels grow and entwine within this mass, making it almost impossible to
operate on without clotting factor. The patient could easily die. Derrick was
lucky; there was clotting factor available, and surgeons at Murang’a removed
the offending mass. Today, he wasn’t home at first, but his grandmother,
Virginia greeted us like we were family, and long lost relatives at that. I was
late joining the group as I ran back to get our bags of goodies from the car. When
I arrived, tripping down the dusty path and onto her farm, she saw me,
recognized me and despite her advanced years, crouched down like a tiger, arms
sprung open and flew at me. We embraced and squeezed each other tight. Then she
immediately launched into a lecture about my weight: why was I so skinny? “Like
you!” I replied. She grabbed me tighter and we laughed. Wow, she is strong!
Our group looked about her small, contained farm,
noting the healthy looking cow, goats and chickens, so different than
Stanley’s. We shared our gifts with the children there, including Tootsie Pops
and balloons. You cannot imagine the joy a simple balloon brings to children
who literally have no toys, not even a crayon. The bright blue and red balloons
contrasted with the earthy colors of the little farm and homestead. The
children chased the balloons and it gave our group a great way to interact with
them. All shyness vanishes when there is a balloon to toss around. I gave
Paris, Derrick’s five-year-old cousin, a teddy bear from my mother, and she
instinctively and promptly tied it to her back in the fashion of African women
who carry their babies on their backs.
Virginia and Susanne
We ducked and went inside Virginia’s home.
Virginia chattered with animation in her delight to see us. She really is a
funny woman. She looked at Rich and Wendy’s two beautiful daughters with a
critical eye, and wanted to know immediately if they were married. They are
only 16 and 20! When she learned they were not, she said in Swahili, “You will
find a husband here!” and we all laughed.
Then she turned to Eric, and demanded, “Where is
your wife?” No boundaries with Virginia!
Her granddaughter, also named Virginia, is a beautiful
Kenyan woman, quiet and demur, holding one-year-old Susanne on her hip. Derrick
then returned home from school, and shyly greeted us. For life on his simple
farm, seeing all these muzungus
(white people) was a surprise!
Derrick had grown tall. And the only remembrance
of his disfiguring pseudotumor was a small, orange scar on his forehead. His
joints were in good shape and he was happy. We shared more toys with him,
learned about school, and played outside a bit with him. All the while we
assessed the condition of the home, farm animals, children, and school
situation. Maureen was concerned about the apparent ring worm on Derrick’s head.
With many hugs and promises to return, we walked
back up to the dirt road, and to the safari jeeps. But Virginia’s mother wanted
to say a prayer for a safe journey, especially up Kilimanjaro. We all bowed her
head as she prayed in Swahili for our safety. Then the children besieged us for
more candy and balloons. I will always remember to travel with balloons from
now on. I forget how easy they are to transport, and how much children enjoy
them.
Laurie Kelley and Peter
On to the next home: Peter Muchoki. This was not
far down the road, and a new place for Peter, who moved into his uncle’s mud
home with his mother Jane and brother Zakayo. His story is poignant: impoverished, no father,
both brothers have hemophilia, and Zakayo suffers from what sounds
like bipolar disorder. The last time we were here, Maureen and I visited Zakayo in
Mathare, the psychiatric hospital in Nairobi. What a sad visit that was; the
wards are bare of anything warm or home-like. By 8 pm, all
the young men are drugged to be quiet and left to sleep on army cots with only a
thin blanket. Zakayo was left there because Jane couldn’t afford to pay his
bill. Without payment, patients are kept until it is paid, sometimes months. In
the meantime, the bill grows… it’s a vicious circle. We paid it and got him
home that night.
Pulling over on the dirt embankment, we
disembarked and saw Peter, tall and thin, not changed much since 5 years ago.
He has the sweetest face and disposition. We shuffled down a short hill to his
uncle’s home, where they all lived. Like most patients, they have a mud-packed
home, dirt floors, no windows, no inner lights, and a steel-corrugated roof. We
crammed in and chatted with the handsome, soft-spoken young man. Yes, he had
finished school, thanks to a scholarship from Save One Life. He is waiting now
for his grades, and will receive a certificate in electrical engineering. His
goal is to secure an “attachment” (internship) with a company and maybe get
hired. Then, if all goes well, open his own repair shop. These are practical
and doable goals and we were pleased to know he had a plan. His health has been
good, though he did miss time from school due to bleeds. He explained to our
group how painful the bleeds can be. “I did not sleep for two nights due to the
pain,” Peter recalled. “It was during exam time and so it was difficult to
focus on school.” As he spoke I could see sympathy register on Wendy’s face,
and those of her daughters.
We shared with Peter that we had some factor just
for him. We could store it at Murang’a Hospital and he could go there to get
it. He wondered if we could possibly get him a fridge, to store the factor at
home. Eventually he will learn to self-infuse. At first we declined; it’s not
his home and maybe they would be asked to leave? Perhaps the uncle wouldn’t
allow the fridge to go with them?
Rich was clearly frustrated with this answer and
wanted to do something now. I love
that attitude! We discussed the fridge with Maureen and Kehio, and they agreed at last. I turned to
the guys—Mike, Rich and Eric—and asked if they could change Peter’s life for
the better right now? Not a problem. Out came $200 and we gave it to Sarah. She
would return in a few days with the money, and shop with the family at the
market, to ensure the money is used for a fridge.
Mission accomplished! Peter is doing well, will
now have factor in his home, an incredibly rare thing in Kenya. He’s our hope
for the future.
No sooner were we in the safari jeeps, then
Zakayo appeared, on crutches. He looked preoccupied, as if in pain. I hopped
out of the jeep, gave him a hug, and asked if he remembered me. He did. Jane
started pulling up his pants leg to show me his wound, a deep gash in the shin,
bleeding through the bandages. Zakayo wanted money, to start a stand to sell
items, possibly fruit, but due to his condition, we didn’t think this was a
good idea. We’d rather support the mother or Peter, who in turn would support
him. He seemed crushed with this answer, and backed away. I wish we could help
each child, but sometimes we cannot.
Still, it was a productive day with many
memories. To each family we pooled our money and gave a cash donation equal to
about half of all their monthly income, just to ease their burdens, which
are many. And each in turn gave us a gift: a huge stalk of bananas, or a bag of
maize, a hug. But the best gift of all was their permission, to allow us to help
them, to allow us to share their world, so different than our own.
Hopefully, we will share our futures with them
through this journey called life.
More stories next week, after our Kilimanjaro climb!
HemaBlog Archives
Categories
LA Kelley Communications - You are leaving our site
You have clicked on one of our advertiser’s links. Our provision of a link to
any other website or location is for your convenience and does not signify
our endorsement of such other website or location or its contents.
Would you like to continue?
Download Now
Would you like to be added to our email list to continue to recieve future editions of PEN in PDF format?


 It is important to plan a meeting with the school staff before the school year is in full swing. If you haven’t done this yet, try to organize a meeting as soon as you can; don’t wait for back-to-school night when teachers will be busy meeting with many parents in one evening.
It is important to plan a meeting with the school staff before the school year is in full swing. If you haven’t done this yet, try to organize a meeting as soon as you can; don’t wait for back-to-school night when teachers will be busy meeting with many parents in one evening. 

 First we stopped at the familiar store we stopped at five years ago, when Eric and I and another group summited Kili, to pick up snacks. We sat about in the sunshine on the grass, waiting for the guides to return. Hesbon went with me across the street to a shop to get a Nalgene bottle, for $7 which he fronted. I don’t think I ever even used the bottle in the end.
First we stopped at the familiar store we stopped at five years ago, when Eric and I and another group summited Kili, to pick up snacks. We sat about in the sunshine on the grass, waiting for the guides to return. Hesbon went with me across the street to a shop to get a Nalgene bottle, for $7 which he fronted. I don’t think I ever even used the bottle in the end. Our first day then had us hiking about six hours to the Machame Camp, elevation 9,927 feet. The route was a groomed trail for the most part, through a dense and moist rain forest. It was cool and progressively dark. The forest was lovely, lush green, with trees covered in soft moss, making them resemble a young deer’s antlers, covered in velvet. Many birds serenaded me. One had a distinct sound: “Tweet… bong!”
Our first day then had us hiking about six hours to the Machame Camp, elevation 9,927 feet. The route was a groomed trail for the most part, through a dense and moist rain forest. It was cool and progressively dark. The forest was lovely, lush green, with trees covered in soft moss, making them resemble a young deer’s antlers, covered in velvet. Many birds serenaded me. One had a distinct sound: “Tweet… bong!”



 We climbed from 8 am until 2 pm, reaching Shira Cave Camp, at 12,355 feet. By now everyone was feeling good, except Mike. But he never complained, and still kept plowing forward on this difficult hike. At 4 pm, Edwin, a cheerful 28-year-old guide, asked us if we wanted to do a 45-minute acclimatizing climb while dinner was prepared. Despite the large number of climbing parties, there was more space at this camp, and we spread out. Eric, Rich, Mike and I all did the acclimatization climb, which was not hard. I felt great at this altitude and relished the climb on the rocks, which were beautiful.
We climbed from 8 am until 2 pm, reaching Shira Cave Camp, at 12,355 feet. By now everyone was feeling good, except Mike. But he never complained, and still kept plowing forward on this difficult hike. At 4 pm, Edwin, a cheerful 28-year-old guide, asked us if we wanted to do a 45-minute acclimatizing climb while dinner was prepared. Despite the large number of climbing parties, there was more space at this camp, and we spread out. Eric, Rich, Mike and I all did the acclimatization climb, which was not hard. I felt great at this altitude and relished the climb on the rocks, which were beautiful.









 We geared up, and began the climb. Again, one of my favorite parts of the trip! My quads are feeling fantastic after all the training I did this summer, hiking Mt. Washington and working with my trainer, Dan French. In fact, I would not use my trekking poles on the entire journey, except for the rapid descent after the summit. So here, I vaulted straight up the wall using my quads and balance. Everyone did well; everyone scaled it and enjoyed photos at the top, where a crystal blue sky greeted us. The view—spectacular. We could see down into the valley. Our camp was now just a colorful speck. Our team was smiling and happy!
We geared up, and began the climb. Again, one of my favorite parts of the trip! My quads are feeling fantastic after all the training I did this summer, hiking Mt. Washington and working with my trainer, Dan French. In fact, I would not use my trekking poles on the entire journey, except for the rapid descent after the summit. So here, I vaulted straight up the wall using my quads and balance. Everyone did well; everyone scaled it and enjoyed photos at the top, where a crystal blue sky greeted us. The view—spectacular. We could see down into the valley. Our camp was now just a colorful speck. Our team was smiling and happy! Onward with no time to lose. We marched down the valley, on slippery, dusty trails that plummeted down at 45° angles at times, maybe even steeper. Our guides held our hands and prevented falls whenever possible. At the bottom, we crossed creeks, jumped rocks, and made it to a flatter surface, dusty with volcanic ash powder, and dotted only occasionally by the oddly placed massive boulder. It was a surreal, primitive, prehistoric landscape. Grey and black base, domed by a brilliant blue ceiling. We were feeling the effects of altitude, which slowed us a bit. Eventually we started to ascend again, up the trails, where flat slabs of shale chimed when we stepped on them, adding a touch of class to the barren landscape.
Onward with no time to lose. We marched down the valley, on slippery, dusty trails that plummeted down at 45° angles at times, maybe even steeper. Our guides held our hands and prevented falls whenever possible. At the bottom, we crossed creeks, jumped rocks, and made it to a flatter surface, dusty with volcanic ash powder, and dotted only occasionally by the oddly placed massive boulder. It was a surreal, primitive, prehistoric landscape. Grey and black base, domed by a brilliant blue ceiling. We were feeling the effects of altitude, which slowed us a bit. Eventually we started to ascend again, up the trails, where flat slabs of shale chimed when we stepped on them, adding a touch of class to the barren landscape. By the time we reached base camp, we were struggling with oxygen, sunburned and elated! This was it. What we came for. What we prepared all year for. The Moment! The entire camp was perched on a mountainside, and before us was the stunning, magnificent Kibo Peak, beckoning us to climb. We could clearly see its white glazed top, its rocky sides. Kili is a beauty of a mountain. I felt awed and honored to be standing before it. I made my way to my tent, ditched my backpack and gear and wandered about till all of our team made it to the camp. My coughing had gotten worse and my voice was hoarse and raspy. Hesbon offered antibiotics as a precaution. My lungs are my Achilles Heel, so I took them. They immediately gave me severe heartburn, so badly I was not able to eat much lunch. This was a bad sign as I would need my energy to summit.
By the time we reached base camp, we were struggling with oxygen, sunburned and elated! This was it. What we came for. What we prepared all year for. The Moment! The entire camp was perched on a mountainside, and before us was the stunning, magnificent Kibo Peak, beckoning us to climb. We could clearly see its white glazed top, its rocky sides. Kili is a beauty of a mountain. I felt awed and honored to be standing before it. I made my way to my tent, ditched my backpack and gear and wandered about till all of our team made it to the camp. My coughing had gotten worse and my voice was hoarse and raspy. Hesbon offered antibiotics as a precaution. My lungs are my Achilles Heel, so I took them. They immediately gave me severe heartburn, so badly I was not able to eat much lunch. This was a bad sign as I would need my energy to summit. But attitude and motivation go a long way, and I was pumped up! Our plan, explained Hesbon to the group, was to have a light dinner, then return to our sleeping bags to catch maybe a few hours of sleep. Then we would depart in two groups: the first was Eric Hill and son Andrew, who proved to be the mountaineers of the group. They could go faster than us and wanted to not have to stop for breaks (stopping for frequent breaks can refuel the climbers but can also allow the cold to settle in, and can actually demoralize the faster climbers who crave to keep moving). Their guide would be Kelvin, and they’d leave at 1 am Thursday morning. Our group was the second group, guided by Victor, including everyone else. We’d leave at midnight. Wendy opted not to summit, which was disappointing to all, but the right decision. She had struggled with asthma and dust the entire day, and it was quite frankly astonishing she was even at base camp. As sweet as she is, the woman has a core of steel!
But attitude and motivation go a long way, and I was pumped up! Our plan, explained Hesbon to the group, was to have a light dinner, then return to our sleeping bags to catch maybe a few hours of sleep. Then we would depart in two groups: the first was Eric Hill and son Andrew, who proved to be the mountaineers of the group. They could go faster than us and wanted to not have to stop for breaks (stopping for frequent breaks can refuel the climbers but can also allow the cold to settle in, and can actually demoralize the faster climbers who crave to keep moving). Their guide would be Kelvin, and they’d leave at 1 am Thursday morning. Our group was the second group, guided by Victor, including everyone else. We’d leave at midnight. Wendy opted not to summit, which was disappointing to all, but the right decision. She had struggled with asthma and dust the entire day, and it was quite frankly astonishing she was even at base camp. As sweet as she is, the woman has a core of steel! I actually was able to get some sleep, though had to pass on dinner, as my stomach burned with the aftereffects of the antibiotics. At 10 pm, I awoke and started planning what to wear to the summit: layers. Incredibly, the weather was mild, at only 20°, with almost no wind. This was a stark contrast to five years ago when it was -5° with 50 mph gusts, freezing us, sapping us of strength, and cloaking any view with white out conditions. We couldn’t get off Kibo fast enough then. This time would be radically different.
I actually was able to get some sleep, though had to pass on dinner, as my stomach burned with the aftereffects of the antibiotics. At 10 pm, I awoke and started planning what to wear to the summit: layers. Incredibly, the weather was mild, at only 20°, with almost no wind. This was a stark contrast to five years ago when it was -5° with 50 mph gusts, freezing us, sapping us of strength, and cloaking any view with white out conditions. We couldn’t get off Kibo fast enough then. This time would be radically different. We gathered in the mess tent and did a gear check. We were each assigned someone to carry our backpack and monitor us. Team Kilimanjaro does a great job of motivating climbers as well as monitoring their physical condition for signs or mountain sickness. Off we went!
We gathered in the mess tent and did a gear check. We were each assigned someone to carry our backpack and monitor us. Team Kilimanjaro does a great job of motivating climbers as well as monitoring their physical condition for signs or mountain sickness. Off we went! The guides forced us to go pole pole. One step, then another, as slow as possible. They also created a rhythm, so important in keeping your pace and momentum. The night was clear and millions of stars burned overhead. It was a night created for a perfect summit! Step, swing, step, swing went our gait. Up, up the rocky path to the summit. I monitored the time and by 1:30 am we had our first break. Hydrating is key, though water tends to freeze in the Camelback tube. I looked upwards at the infinite sky and saw constellations: Orion the Hunter, Taurus, and then Cassiopeia, shaped like a W. The W was upside down, forming an M (for mountain?) over Kibo, and it guided me through the night. Twice I saw shooting stars, like fireworks celebrating our summit. I took the time to take out my iPod and started playing music to keep me going. Five years ago I lost track entirely of the night, and 7 hours merged into memories of only about an hour. Not this time: I played about three hours of Metallica and the Doors, and then Guns N’ Roses. At 5 am, I was actually dancing with the porters on the mountain, gyrating as they sang, then playing air guitar to Welcome to the Jungle….
The guides forced us to go pole pole. One step, then another, as slow as possible. They also created a rhythm, so important in keeping your pace and momentum. The night was clear and millions of stars burned overhead. It was a night created for a perfect summit! Step, swing, step, swing went our gait. Up, up the rocky path to the summit. I monitored the time and by 1:30 am we had our first break. Hydrating is key, though water tends to freeze in the Camelback tube. I looked upwards at the infinite sky and saw constellations: Orion the Hunter, Taurus, and then Cassiopeia, shaped like a W. The W was upside down, forming an M (for mountain?) over Kibo, and it guided me through the night. Twice I saw shooting stars, like fireworks celebrating our summit. I took the time to take out my iPod and started playing music to keep me going. Five years ago I lost track entirely of the night, and 7 hours merged into memories of only about an hour. Not this time: I played about three hours of Metallica and the Doors, and then Guns N’ Roses. At 5 am, I was actually dancing with the porters on the mountain, gyrating as they sang, then playing air guitar to Welcome to the Jungle….

 And then the iPod died. I knew from then on it would be a struggle. While hoping to summit at 7, our group was slow. This was good as no one got sick, but it depleted that much more energy. The guides forced Red Bull down us, which I detest but drank. It instantly gave us energy. Stinger waffle snacks, Gu gel, hot tea, anything to keep us energized. But the energy drained away. I bonked. I had been running on music and fumes and now my music was gone. It did a psychological number on me. Why didn’t I keep a second iPod in my other pocket! (Note to self for next time…)
And then the iPod died. I knew from then on it would be a struggle. While hoping to summit at 7, our group was slow. This was good as no one got sick, but it depleted that much more energy. The guides forced Red Bull down us, which I detest but drank. It instantly gave us energy. Stinger waffle snacks, Gu gel, hot tea, anything to keep us energized. But the energy drained away. I bonked. I had been running on music and fumes and now my music was gone. It did a psychological number on me. Why didn’t I keep a second iPod in my other pocket! (Note to self for next time…)
 We needed to get down as oxygen is only 50% at the summit. We linked up one by one: Jim, Mike, Rich, Samantha, Taylor, me, our guides, and started the descent. Eric and Andrew were already on their way down. This would take over 5 hours and was another punishing trip. But for now, we gleefully focused on the goal we achieved and worked so hard for: the summit. Somewhere in my oxygen-deprived head, I was also thinking of what this could mean for Save One Life and the patients we serve. Money for programs; motivation to keep persevering despite setbacks and challenges; and perhaps, another summit climb, when more captains of industry like Rich, Eric and Mike join us to experience the outer limits of endurance, to raise money and awareness for hemophilia in developing countries, and to triumph, personally and professionally. When there is a common cause to help others who suffer, a purpose bigger than ourselves there seems to be no limits to what a group of compassionate people can accomplish.
We needed to get down as oxygen is only 50% at the summit. We linked up one by one: Jim, Mike, Rich, Samantha, Taylor, me, our guides, and started the descent. Eric and Andrew were already on their way down. This would take over 5 hours and was another punishing trip. But for now, we gleefully focused on the goal we achieved and worked so hard for: the summit. Somewhere in my oxygen-deprived head, I was also thinking of what this could mean for Save One Life and the patients we serve. Money for programs; motivation to keep persevering despite setbacks and challenges; and perhaps, another summit climb, when more captains of industry like Rich, Eric and Mike join us to experience the outer limits of endurance, to raise money and awareness for hemophilia in developing countries, and to triumph, personally and professionally. When there is a common cause to help others who suffer, a purpose bigger than ourselves there seems to be no limits to what a group of compassionate people can accomplish.
















