Learn about bypassing agents: a factor option with a long history of use

Inhibitors can be a devastating response to infused factor. It’s good to review what they are, how they form, and what treatment is available, even if you or your loved one do not have an inhibitor. Below is information on what we know about inhibitors.
Read and learn!
Laurie
This is a paid public announcement from Shire and does not constitute an endorsement of products or services. When you click on the links in this blog entry, you will be directed to the Shire website. LA Kelley Communications always advises you to be a savvy consumer when contacting any company; do not reveal identifying information against your will.
The development of inhibitors adds great challenges to managing hemophilia
As you may know, factor proteins are a vital component in the blood-clotting process and help to stop or control bleeds. However, if you are missing one or more of these factors, your body is unable to effectively manage a bleed.1-3 Factor treatment temporarily replaces the missing proteins in your blood, working within the natural blood-clotting process to help create the necessary clot and stop a bleed.1-6
Treatment of inhibitors is one of the greatest challenges in hemophilia today.7 Some patients develop antibodies called inhibitors that actually stop, or block, factor VIII (FVIII) or factor IX (FIX) function in the blood-clotting process.8,9 In fact, up to 33% of people with severe hemophilia A develop an inhibitor to treatment, while 5% to 10% of patients with mild to moderate hemophilia A develop an inhibitor.9-11Inhibitors are less common among people with hemophilia B, affecting only 1% to 6% of individuals. Bleeding is more difficult to manage in patients with inhibitors because they do not respond to standard factor replacement treatment. Inhibitors attach to the replacement factors, making the treatment ineffective.11
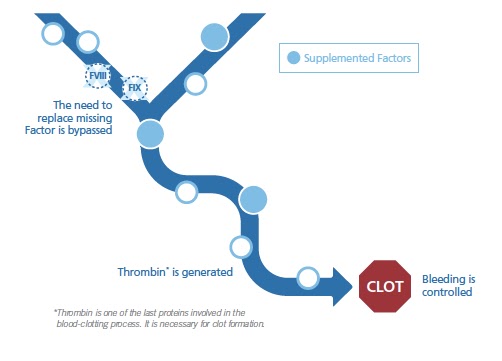
To avoid the need to replace missing factors, patients with inhibitors need a different treatment approach, such as the use of bypassing agents. Bypassing agents are made up of factor, or a combination of factors that are naturally found in the body’s blood-clotting process. Bypassing agents offer an alternative treatment approach because they go around, or bypass, the need for FVIII or FIX while supplementing factors involved in the blood-clotting process.8,11-14
This chart is a simplified visualization of Bypassing Agent activity in the blood clotting process.
One way to think about the role of bypassing agents in the blood-clotting process is to compare it to a light switch:
 |
Activation
Turning the light switch on—Before a bleed occurs, the process remains off but available when needed. When a bleed begins, the process is turned on. After infusion, bypassing agents are available to help control/manage the bleed.
|
 |
Inactivation
Turning the light switch off—Once the bleed is managed, the blood-clotting process is inactivated.
The unused bypassing agent factors are eliminated from your blood. This inactivation step is very important. Unchecked thrombin generation could lead to risk of blood clots over time.
|
By working within the body’s natural mechanisms, bypassing agents are able to help stop a bleed in 3 tailored ways: when the bleed occurs, where (the site of the bleed), and how—by helping to form a more stable clot to help control the bleed.12,15
Bypassing agents provide options for individualized treatment.1 Currently, there are 2 bypassing agents available to treat people with inhibitors, and response to either treatment option may vary.15,16 In a study published in the peer-reviewed journal Blood, it was shown that 60% to 67% of people responded in the same way to each bypassing agent. These patients either responded to both bypassing agents or did not respond to either bypassing agent. However, up to 40% of people responded to only one bypassing agent and not the other in the first 12 hours after an infusion. The difference in patient response reduced from 7.3% after 48 hours.17
There are serious risks of blood clots with the use of bypassing agents.15 You should be monitored for the development of blood clots. If you experience any side effects while using a bypassing agent, call your healthcare provider right away.
Bypassing agents are infused intravenously, making the proteins needed for clotting immediately available for use.1,12,18,19 Bypassing agents may be used in the following scenarios:
|
PROPHYLAXIS
Infuse routinely to prevent bleeds1 |
ON DEMAND
Infuse when needed or to control breakthrough bleeds1 |
SURGERY
Infuse to prevent/manage bleeds during or after surgery 8, 20 |
It is important to work with a healthcare provider to develop an individualized treatment plan. A healthcare provider can tailor the dose and frequency of bypassing agents to fit with your lifestyle, depending on the severity of a bleed or the type of surgery. For example, if you have a mild bleed, or a minor surgery, your healthcare provider may adjust your dosage and/or frequency of bypassing agents accordingly. If the bleed is more severe, or you are having a major surgery, then your dosage and/or frequency would be increased accordingly.8,15,20
Bypassing agents are backed by a long history of use. Healthcare providers and patients have consistently relied on bypassing agents for over 40 years.21,22 With substantial bleed reduction benefits and extensive clinical experience, bypassing agents are considered a well-studied and established treatment option for hemophilia patients with inhibitors.15,21-23
Shire has been dedicated to pursuing advancements in hemophilia for more than 60 years.24 As a leader and innovator in hemophilia research, we offer a vast array of patient programs and support—all of which are proudly brought to you by our dedicated people.
EXPLORE THE POSSIBILITIES: To learn more about the treatment of patients with hemophilia A with inhibitors using bypassing agents, talk to your healthcare provider.
For more information, you can visit:
http://www.bleedingdisorders.com/bleeding-disorders-info/
http://www.hemophilia.org
http://www.wfh.org
http://www.hemophiliafed.org/
http://www.bleedingdisorders.com/bleeding-disorders-info/
http://www.hemophilia.org
http://www.wfh.org
http://www.hemophiliafed.org/
REFERENCES
| 1. | Peyvandi F, Garagiola I, Young G. The past and future of haemophilia: diagnosis, treatments, and its complications. Lancet. 2016;388:187‐197. |
| 2. | Antovic A, Mikovic D, Elezovic I, Zabczyk M, Hutenby K, Antovic JP. Improvement of fibrin clot structure after factor VIII injection in haemophilia A patients treated on demand. Thromb Haemost. 2013;111(4):656‐661. |
| 3. | Hvas AM, Sørensen HT, Norengaard L, Christiansen K, Ingerslev J, Sørensen B. Tranexamic acid combined with recombinant factor VIII increases clot resistance to accelerated fibrinolysis in severe hemophilia A. 2007;5:2408‐2414. |
| 4. | Johari V, Loke C. Brief overview of the coagulation cascade. Dis Mon. 2012;58:421‐423. |
| 5. | Lenting PJ, van Mourik JA, Mertens K. The life cycle of coagulation factor VIII in view of its structure and function. Blood. 1998;92(11):3983‐3996. |
| 6. | Factor Replacement Therapy. Canadian Hemophilia Society. http://www.hemophilia.ca/en/bleeding-disorders/hemophilia-a-and-b/the-treatment-of-hemophilia/factor-replacement-therapy/. Accessed December 1, 2017. |
| 7. | World Federation of Hemophilia. What are inhibitors? https://www.wfh.org/en/sslpage.aspx?pid=651. Accessed November 9, 2017. |
| 8. | Leissinger CA. Prevention of bleeds in hemophilia patients with inhibitors: emerging data and clinical direction. Am J Hematol. 2004;77(2):187‐193. |
| 9. | World Federation of Hemophilia. Guidelines for the management of hemophilia, 2nd ed. World Federation of Hemophilia, Montreal, Quebec, 2012. |
| 10. | DiMichele DM. Inhibitor treatment in haemophilias A and B: inhibitor diagnosis. Haemophilia. 2006;12(suppl 6):37-42. |
| 11. | DiMichele DM. World Federation of Hemophilia website. Inhibitors in hemophilia: a primer. http://www1.wfh.org/publication/files/pdf‐1122.pdf. Published 2008. Accessed November 9, 2017. |
| 12. | Ananyeva NM, Lee TK, Jain N, Shima M, Saenko EL. Inhibitors in hemophilia A: advances in elucidation of inhibitory mechanisms and in inhibitor management with bypassing agents. Semin Thromb Hemost. 2009;35(8):735‐751. |
| 13. | Retzios AD. The new and improved (?) activated factor VII molecules. Bay Clinical R&D Services. 2001:1-41. |
| 14. | Berg JM, Tymoczko JL, Stryer L. Many enzymes are activated by specific proteolytic cleavage. In: Biochemistry. 5th ed. New York, NY: WH Freeman; 2002. https://www.ncbi.nlm.nih.gov/books/NBK22589/. Accessed November 9, 2017. |
| 15. | Shapiro AD, Hedner U. Advances in bypassing agent therapy for hemophilia patients with inhibitors to close care gaps and improve outcomes. Ther Adv Drug Saf. 2011;2(5):213‐225. |
| 16. | Hoffman M, Dargaud Y. Mechanisms and monitoring of bypassing agent therapy. J Thromb Haemost. 2012;10:1478‐1485. |
| 17. | Astermark J, Donfield SM, DiMichele DM, et al. A randomized comparison of bypassing agents in hemophilia complicated by an inhibitor: the FENOC Study. Blood. 2007;109(2):546‐551. |
| 18. | Hemophilia Federation of America. Treatment of hemophilia. http://www.hemophiliafed.org/bleeding‐disorders/hemophilia/treatment/. Accessed November 9, 2017. |
| 19. | Hedner U. Recombinant activated factor VII: 30 years of research and innovation. Blood Rev. 2015;29(suppl 1):S4‐S8. |
| 20. | Santagostino E, Escobar M, Ozelo M, et al. Recombinant activated factor VII in the treatment of bleeds and for the prevention of surgery related bleeding in congenital haemophilia with inhibitors. Blood Rev. 2015;29(suppl 1):S9‐S18. |
| 21. | Mehta R, Parameswaran R, Shapiro AD. An overview of the history, clinical practice concerns, comparative studies and strategies to optimize therapy of bypassing agents. Haemophilia. 2006;12(suppl 6):54‐61. |
| 22. | National Hemophilia Foundation. Medical and Scientific Advisory Council (MASAC) recommendation regarding the use of bypassing agents in patients with hemophilia A or B and inhibitors. MASAC document #167. 2006. |
| 23. | NIH Clinical Trials Registry. Ongoing and complete clinical trials using bypassing agents in hemophilia patients with inhibitors. https://clinicaltrials.gov/ct2/results/detailsterm=hemophilia+a+with+inhibitors%2C +hemophilia+b+with+inhibitors&recr=Closed&cond=hemophilia+a+with+inhibitors%2C+hemophilia+b+with+inhibitors. Accessed November 9, 2017. |
| 24. | Higgins MC. Career imprints: creating leaders across an industry. 2005. |
S36468 12/17