Both the Royals and the Russians have been making the news this past year, not much of it good. For the Royals, it’s mostly just the Markles (on their “Privacy Tour”). For Russia…. well, let’s not go there.
While Russia is making a ruinous name for itself these past two years, it’s famous for its hemophilia history. Which originated from the English Royals.
We noted last week that it’s Bleeding Disorder Awareness Month, and we shared some popular myths about hemophilia. One was that hemophilia has been dubbed “The Royal Disease.” I shared in detail how this happened, and who it affected in my blog here.
But the most famous outcome of a genetic link in the English Royal family happened when Princess Alix, whose grandmother was Queen Victoria, a carrier of hemophilia B, married Tsar Nicholas II of Russia. Queen Victoria had nine children, of whom two were carriers (Alice and Beatrice) and one had hemophilia (Leopold). It was well known that hemophilia was now running in the family.
Alix, nicknamed “Sunny” by Nicolas, gave birth to Alexis (or Alexei), after already having four girls. They got their heir to the throne. But Alexis had hemophilia.
Alexis had no access to clotting factor of course; this was 1904, after all. The royal family came rely on a person of ill repute: Rasputin, the mad monk. He had a lascivious reputation but also a track record of helping people in pain, probably through hypnosis. Rasputin became ingratiated into the royal family and helped also to bring down the Russian monarchy. It’s been proposed that Nicholas II was so distracted by his son’s suffering due to hemophilia, that eventually he lost his grip on the monarchy at a time when the Bolshevik Revolution was poised to strike. And it did. It has been proposed that hemophilia changed the course of World War I, and changed the course of history. The Cold War, the Soviet Empire… all find their roots in the royal palace of the Tsar and a little boy with hemophilia.
It’s Bleeding Disorder Awareness Month! True: Designated in 1986 as Hemphilia Awareness Month this is the month to educate the public—and ourselves—about bleeding disorders.
I usually start with what hemophilia is not. Perhaps because hemophilia is so rare, it has generated many myths. Myths are stories, sometimes created by people in an attempt to make something understandable when scientific information is unavailable. Remember the Greek tale of Pandora’s Box? Pandora was the first woman on earth. She was given a wedding gift from the gods, a beautiful container. But she was warned never to open it. Driven by curiosity, she disobeyed the gods and opened it. Inside were evils—hate, disease, pain—that flew out of the container and escaped into the world. This story was invented by the ancient Greeks to explain sickness and suffering, because they didn’t know about bacteria and viruses. Some myths develop from a nugget of fact or experience, but then take on a life of their own within certain cultural settings.
Becoming familiar with the most widely held myths about hemophilia and their sources will help you explain the facts of the disorder to others. Here are some common myths about hemophilia.
Truth: Anyone can get hemophilia—rich or poor, famous or unknown. Hemophilia was dubbed the royal disease because in the 1800s, hemophilia affected the family of Queen Victoria of England, who was a carrier of the hemophilia gene. Hemophilia was transmitted to three other royal families when Victoria’s daughters and granddaughters, also carriers, married into the Russian, German, and Spanish royal families. Though it’s no longer known to be present in any European royal family, hemophilia is still often associated with royalty.
Myth: A small cut will cause blood to rush out and a child to bleed to death.
Truth: People with hemophilia do not bleed faster than anyone else. But they will bleed longer because their blood doesn’t clot properly. Still, not every cut will continue to bleed just because a person has hemophilia. Some cuts, especially small ones, stop bleeding on their own.
Myth: Children with hemophilia cannot play sports.
Truth: Children with hemophilia enjoy a wide variety of sports, including swimming, baseball, tennis, running, and martial arts. You’ll realize this someday when you’re chauffeuring your sports fan to various afterschool activities! High-impact contact sports such as football, hockey, and boxing are not advised. Physical activity is always encouraged for children with hemophilia.
Myth: Children with hemophilia must wear helmets and protective gear.
Truth: Although some parents place protective helmets or knee pads on their toddlers, it’s uncommon for a child with hemophilia to wear protective gear for normal activities. Medical treatments today are excellent and easy, offering a normal lifestyle. Of course, all children must wear protective gear when participating in risky activities: helmets should always be worn when riding bikes or motorcycles, ores, or when skiing or snowboarding. Oh yes, your child will be able to do these things one day!
Myth: Children with hemophilia must attend a special needs school.
Truth: Except for having a defective blood protein for blood clotting, our children have normal health and intelligence. They can be enrolled in any school. Overall, your child is normal and will be treated as such by the school system and the public.
Myth: Children with hemophilia need to be placed in special schools or classes.
Truth: Except for having a defective blood protein for blood clotting, our children have normal health and intelligence. They can be enrolled in any school. Overall, your child is normal and will be treated as such by the school system and the public.
Myth: Children with hemophilia will grow out of it.
Truth: Hemophilia is a lifelong condition. Your child does not have a disease that will get better or go into remission. Your child will not grow out of hemophilia: the mechanism for producing clotting factor is defective. Hemophilia is part of his genetic makeup, just like traits for hair or eye color, which can’t be outgrown. However, there is now a genetic therapy available for hemophilia B that will give, with one shot, protection against uncontrollable bleeds for a long time.
Myth: Hemophilia is caused by something you did during pregnancy.
Truth: Nothing you did while pregnant gave your baby hemophilia. Women who have perfect pregnancies and follow every safety precaution can give birth to children with hemophilia. There’s nothing you could have done to prevent hemophilia; nor could you have changed your child’s hair or eye color. Hemophilia is simply part of his genetic makeup.
Don’t feel guilty; get educated, and educate others. Now’s the month especially to do this!
Hemophilia—all bleeding disorders really—requires help, and not just from therapies. Due to healthcare changes, patients are required often to pay higher out of pocket costs. And sometimes, it’s just life: single parenting, limited job opportunities, higher education bills, gas, care and health insurance. We could all use help.
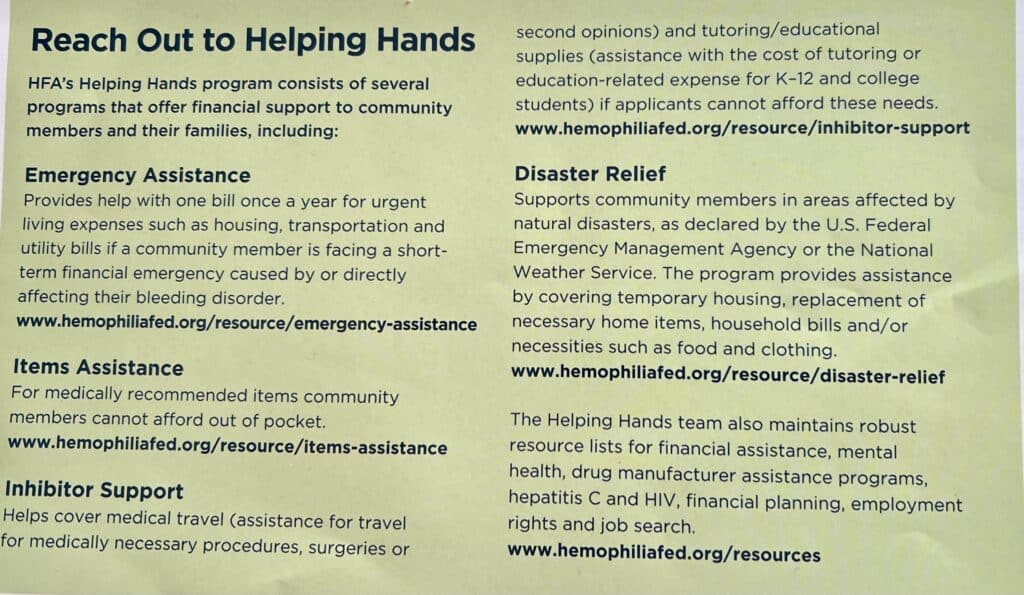
Hemophilia Federation has a great listing of all their ways they might help. HFA has long impressed me with their direct-to-patient aid. It’s a lot like what we do with Save One Life overseas: we give direct aid to those most in need. You local chapter might be a good first place to start, but then look at HFA’s website to learn more.
Check out these opportunities and find out if you are eligible:
I’m here in Antarctica, and have visited the grave site of one of the most famous leaders in history: Ernest Shackleton. The famed polar explorer was renowned for surviving a horrendous situation, and leading the men directly under his watch to safety. It’s such a compelling story, that I had to come to the Antarctic after reading in depth about it for years!
Ernest Shackleton
The bleeding disorder community is filled with admirable leaders, too. Though I often say that no one is a born leader, leadership can be birthed. In our community, leadership arose from the cataclysmic devastation when HIV was discovered in the blood supply in the 1980s and infected about half of our community. This horrific event birthed many leaders, whose legacies stand today.
When we think of those leaders—like Corey Dubin, Dana Kuhn, Val Bias, Jeanne White-Ginder, and Louise Ray—we think of certain leadership qualities: vision, authority, courage, commitment. These are leaders who made history and secured a safer future for us all.
Yet today, when you ask regular moms and dads and hemophilia patients about leadership, a slightly different picture emerges, highlighting different qualities. It helps to know more about what our community members seek today in leadership—who they admire, and what they expect from the leadership of tomorrow.
Types of Leadership
There are many types of leadership, but I usually peg leaders as one of three types: positional, situational, and transformational. In a nutshell, positional leaders are usually elected, appointed, or inherited: think president, CEO, executive director, chief, even king or queen. Situational leaders may or may not be positional leaders, but they rise to the forefront when a problem, event, or situation calls for a leader. Think first responder, rescuer, or anyone who steps forward to take action, like Lech Walesa of Poland in 1980, or US Army Major Hugh Thompson, Jr., during the Vietnam War. Or even Ripley in Alien!
Transformational leaders influence a community, industry, group, or era to make massive and lasting changes: think Jesus, Gandhi, Walt Disney, or Steve Jobs. When asked about leaders, people often name leaders who fall into those three categories. Characteristics of these types of leaders? Powerful, authoritative, visionary, action-oriented, decisive, committed, communicative, innovative, influential, even charismatic. Do bleeding disorder families see leadership the same way?
The Softer Side of Leadership
Rather than describe leaders in our community as figureheads with power and influence, parents and patients associate softer qualities with leaders these days. These softer qualities include traits that make the “followers,” or beneficiaries of leadership, feel more secure and feel their needs are being met. We polled parents and patients on Facebook to see what leadership qualities they look for most in the bleeding disorder community. And top among these qualities is listening.
Eva replied, “For me, a good quality of leadership is to have an ear to listen, to communicate. To protect their member.” Krissy agreed. “Leadership is the ability to not just listen but truly hear you and your concerns. A leader inspires others and is someone who advocates passionately.”
Dr. Anupama Pattiyeri of India added that a leader must be “a patient listener and motivator—someone who focuses on solutions and not on problems alone.” Katelyn and Alicia both put listening as their first sign of good leadership.
Wayne remarked that leadership means “the ability to listen before deciding. Having ties to the community and leading with integrity, honesty and compassion.” Karla agreed; for her, leadership means “commitment to our community combined with a personal connection.”
Tina noted that listening, combined with empathy, insight, and integrity, gives a leader the ability to understand life from a patient’s or caregiver’s point of view; the ability to understand important values of the community; and “the strength to stand up for those values.” In other words, parents and patients view the traditional forms of leadership as less important than “servant” leadership.
Servant Leadership
The style of leadership parents and patients most often mentioned is known as servant leadership. Servant leadership puts people’s needs first. A leader must understand the needs of the followers or constituents, be there with them, even suffer with them. Indeed, a trait of servant leadership is compassion, which means to suffer or feel alongside someone. It follows that traits of servant leaders include listening, empathy, stewardship, awareness, healing, commitment, and community-building. Historically, servant leaders have been either positional, situational, or transformational leaders too, but have always put their people’s needs first.
Ray agreed. “To be in service to the people you are leading—servant leadership” explains the style of leadership that works best today in our community.
Who are the servant leaders in the bleeding disorder community? Kathe cited her HTC physicians: “Both physicians are excellent leaders…They always take time to explain to patients and integrate therapies into everyday life. I am a better nurse for knowing them.” Rayna mentioned her doctor, currently at St. Jude’s, “for leading a whole generation of patients through recombinant therapies by studying the medicine and checking the facts. All the while he has a wonderful bedside manner to both parents and children.”
Kelly, who was nominated by respondents as a servant leader herself, listed integrity, compassion, and honesty as important qualities for our community leaders. These characteristics don’t require a leader to be in a position of authority.
But positional leaders—those in authority—can be servant leaders as well. Christal nominated a couple who started a chapter in her state, and do so much to help the underserved members of our community.
Likewise, Tiffany recommended Sue Martin, executive director of Hemophilia of South Carolina, as a servant leader. “She gives our organization her heart and soul. She has turned our local chapter into a source of hope, progression and compassion for our bleeding disorders community. And most importantly she drives people to educate themselves on advocacy, so we can advocate strongly and effectively for our children, and teach them how to become strong advocates for themselves.”
Ray warned that as great as servant leaders are, they must ensure that they are not indispensable. In other words, leaders must develop other leaders.
Mentoring
The great British wartime leader Winston Churchill was called the “Old Lion.” I think of this when I think of the top leaders in our community who fought our war with HIV, and are now in their 60s. Mentoring a new generation of lions, then, is vital. Some mentoring happens at the top, with youth leadership programs from National Hemophilia Foundation (NHF), but mentoring can occur anywhere by any of our servant leaders.
Two mothers mentioned their own sons as servant leaders who mentor younger followers. One mentioned that her son never missed a year of summer camp since age seven, and even after moving out of state for a while, came back to work as a counselor in summers. Servant leadership by example, combined with positional leadership, is powerful!
Kimberly nominated her son, who she believes has these leadership qualities, so important in servant leaders: integrity, honesty, loyalty, empathy, compassion, inspiration—and mentoring.
Unsung Heroes
Finally, Lisa made a poignant suggestion: “I’d like to nominate all of the ‘silent leaders’…parents who take the time, often in private, to welcome new members, offer our help, guidance, experience as parents with a baby with a bleeding disorder…Often done behind the scenes, but very helpful and appreciated nonetheless.”
Sometimes the greatest leaders are the ones without the fanfare, tweets, photo ops, and popular achievements. They are the servant leaders who quietly and modestly, powerfully and permanently, change the world day by day, child by child. They are all of you—parents, patients, doctors, nurses—who dedicate their lives and careers to the bleeding disorder community.
The collective pursuit to control the spread of coronavirus resulted in an enormous challenge for the bleeding disorder community. The economic fallout of sheltering in place has affected our need for a steady income, health insurance, access to medical treatment, and—equally important—our access to each other. The degree of impact on our families is hard to determine, but it’s safe to say this pandemic has been very stressful.
But stress in not a new concept for the bleeding disorder community. In fact, our community has been dealing for years with the emotional angst of fighting for what is needed to manage our medical conditions. Remember our fight for safer products, or our fight for laws to protect us from job discrimination? Today’s battle, for our community, is to deal with the stress resulting from the pandemic. So let’s follow the same steps we have taken so many times before. Let’s get informed, find our resources, and stick together.
Get Informed
To learn to manage stress, we need to become familiar with how our central nervous system works. Our brain comes pre-wired with an intricate system that functions to keep the rest of our body alive. This is the limbic system, which provides the “fight-or-flight” response. If the brain determines that the body is in danger, it initiates a chemical chain reaction that gets the body ready to either fight the challenge or run from it. This response begins when sensory information is picked up by a part of the brain called the amygdala. If the amygdala determines there is a threat, it signals other parts of the brain and body to release hormones such as adrenaline and cortisol. These hormones instruct the heart and lungs to increase their output in order to create the energy needed to meet the challenge. This fight-or-flight response is extremely effective when a person needs physical energy to avoid a danger such as jumping out of the way of a car. But most of today’s challenges are emotional, and they don’t require the extra energy provided by the stress response. The result is a steady supply of stress hormones circulating in the body at all times. The image that comes to mind is a person standing next to an IV pole and steadily receiving drips of adrenaline and cortisol. In others words, our body remains in a constant state of high alert.
The good news: We do have the ability to slow down the stress response. Since we now know that the brain is constantly scanning our body and our environment to determine if it should go into stress or relaxed mode, we can intentionally offer cues to indicate that we’re not in danger. In fact, this is how meditation works. The first goal of meditation is to slow down your breathing rate. This is important, because once your brain receives the signal that your breathing rate is lowered, it will interpret this to mean that you’re not in danger, and will turn off the stress response. The second goal of meditation involves your focus. You want to be focusing on the present—instead of musing about the past or anticipating the future—and you want to intentionally focus on words or images that evoke feelings of peace or happiness.
You can bring up images of when you felt safe and happy, or you can think of words that reassure you. This tool is like anything else in life: it requires practice and commitment. But eventually, you’ll find that you can truly create a sense of well-being, no matter what’s going on in your life. Sound too good to be true? Do you need proof? Ask yourself how you feel when you’re watching a scary movie, and compare that to how you feel when you’re watching a romantic comedy. In other words, what we focus on creates how we feel inside. That same principle is at work when we intentionally think about what we are grateful for, as opposed to what we lack or what we don’t like about our lives.
Learning to handle stress is more important than ever. Let’s look at the many resources that have been created since the coronavirus pandemic started.
Find Resources
National Hemophilia Foundation (NHF) and Hemophilia Federation of America (HFA) have created content to help people in the bleeding disorder community deal with both physical and emotional impacts of the pandemic. Visit:
And yes, there is an app for learning to relax! Appropriately called the Calm app, it has hundreds of meditations and master classes on stress management: calm.com
It didn’t take long for our community to figure out how to be connected virtually. Though it isn’t the same as being in a room together, it is nice to see familiar faces and get a chance to let someone know you are there for them.
Take a moment to check in with yourself, because it’s very easy to feel lonely in isolation. If you find that you’re exceptionally lonely, depressed, or anxious, it always helps to talk to someone trained to help you feel understood and supported. Online platforms like Talk Space and Better Help are reporting an exponential increase in the number of requests for counseling sessions right now.
One of the best ways to combat the feeling of helplessness that comes with a crisis is to look for a way you can help others. This sense of purpose gives people some control, and helps them feel productive and useful. For me, contributing to Save One Life is one way I fulfill my need to have purpose in my own life. Each month, I have a small sense of satisfaction knowing that there are three young people with hemophilia who feel that someone else on this planet sees them and cares about them.
Look for Purpose
So, whether it’s meditating, talking with someone, or just being there for another human, there are ways to combat stress. We will get through this pandemic as a community, the way we always have. We will get informed, find resources, and seek out each other.
Debbie de la Riva, LPC, has been an active member of the bleeding disorder community since the birth of her son with severe hemophilia 25 years ago. She served as executive director of the Lone Star Chapter of NHF, was a co-chair of an NHF Annual Meeting, received a Ryan White Award for Advocacy Excellence, and has presented on mental health issues to chapter and national organizations. In 2018, Debbie founded Mental Health Matters Too as a way of combining her degree as a licensed professional counselor with her passion for helping community members who struggle with mental health challenges. To contact Debbie: www.mentalhealthmatterstoo.com or debbie@mhmtoo.com
HemaBlog Archives
Categories
LA Kelley Communications - You are leaving our site
You have clicked on one of our advertiser’s links. Our provision of a link to
any other website or location is for your convenience and does not signify
our endorsement of such other website or location or its contents.
Would you like to continue?
Download Now
Would you like to be added to our email list to continue to recieve future editions of PEN in PDF format?