admin
August 12, 2018
The following is sponsored by Shire. Change is good, unless it affects your treatment. Here, we bring you interesting facts about Shire’s products…and reputation as an industry leader. While companies can undergo name changes in our community’s long history, the products remain the same, as does Shire’s commitment to patients.
Laurie
This is a paid public announcement from Shire and does not constitute an endorsement of products or services. When you click on the links in this blog entry, you will be directed to the ADVATE ® [Antihemophilic Factor (Recombinant)] website. LA Kelley Communications always advises you to be a savvy consumer when contacting any company; do not reveal identifying information against your will.
 For over 7 decades, the rare bleeding disorders teams that are now part of Shire have worked toward transforming ideas into products that have the potential to change the lives of patients by reducing bleeds.1,2
For over 7 decades, the rare bleeding disorders teams that are now part of Shire have worked toward transforming ideas into products that have the potential to change the lives of patients by reducing bleeds.1,2
ADVATE ® [Antihemophilic Factor (Recombinant)] was one of those ideas, and in 2003, it was introduces as the first recombinant factor VIII free of blood-based additives. ADVATE is not used to treat von Willebrand disease; do not use ADVATE if you are allergic to mice or hamsters or to any ingredients in ADVATE.3-5
In 2011, ADVATE was approved for routine prophylaxis in adults and children with hemophilia A.3 Did you know that in a clinical study ADVATE reduced bleeds by 98% when patients switched from on-demand to prophylaxis?3,6
What is Prophylaxis in Hemophilia A?
Prophylaxis refers to regular infusion of clotting factor concentrates to help prevent bleeds from occurring.7 In the case of hemophilia A, one option is taking ADVATE prophylaxis to try and help prevent a bleed from occurring.3
In a clinical study:
- There was a 98% reduction in bleeds (median annual bleed rate [ABR] from 44 to 1^1 †) when patients switched from on-demand to prophylaxis3,6
- Patients experiences a 97% reduction in joint bleeds (from 38.7 to 1 median joint ABR) after switching from on-demand to prophylaxis3
- 42% of patients experiences zero bleeds during 1 year of prophylaxis with ADVATE (22 out of 53 patients in the per-protocol* group)3
The clinical study mentioned above was a multicenter, open-label, prospective, randomized, 2-arm, controlled postmarketing clinical study of the relative efficacy of ADVATE use in 2 prophylactic treatment regimens compared to that of on-demand treatment; 53 previously treated patients (PTPs) with severe to moderately severe hemophilia A (FVIII level <2 IU/dL) were analyzed in the per-protocol group. Subjects were initially treated for 6 months of on-demand therapy and then randomized to 12 months of either a standard prophylaxis regimen (20-40 IU/kg every 48 hours) or a pharmacokinetic-driven prophylaxis regimen (20-80 IU/kg every 72 hours). ABRs for the two prophylaxis regimens were comparable.3,6
You should also know important safety information about ADVATE, such as symptoms of an allergic reaction to ADVATE, that your body may form inhibitors to factor VIII that may stop ADVATE from working properly, and the most common side effects.3 See additional safety information below this video and talk to your doctor to see if ADVATE may be right for you.

Want to learn more about how we do it? We went to one of our manufacturing facilities to show you just how much detail goes into each little vial.
Watch it here.
ADVATE [Antihemophilic Factor (Recombinant)] Important Information
What is ADVATE?
- ADVATE is a medicine used to replace clotting factor (factor VIII or antihemophilic factor) that is missing in people with hemophilia A (also called “classic” hemophilia).
- ADVATE is used to prevent and control bleeding in adults and children (0-16 years) with hemophilia A. Your healthcare provider (HCP) may give you ADVATE when you have surgery.
- ADVATE can reduce the number of bleeding episodes in adults and children (0-16 years) when used regularly (prophylaxis).
ADVATE is not used to treat von Willebrand disease.
DETAILED IMPORTANT RISK INFORMATION
Who should not use ADVATE?
Do not use ADVATE if you:
- Are allergic to mice or hamsters.
- Are allergic to any ingredients in ADVATE.
Tell your HCP if you are pregnant or breastfeeding because ADVATE may not be right for you.
What should I tell my HCP before using ADVATE?
Tell your HCP if you:
- Have or have had any medical problems.
- Take any medicines, including prescription and non-prescription medicines, such as over-the-counter medicines, supplements or herbal remedies.
- Have any allergies, including allergies to mice or hamsters.
- Are breastfeeding. It is not known if ADVATE passes into your milk and if it can harm your baby.
- Are or become pregnant. It is not known if ADVATE may harm your unborn baby.
- Have been told that you have inhibitors to factor VIII (because ADVATE may not work for you).
What important information do I need to know about ADVATE?
- You can have an allergic reaction to ADVATE. Call your HCP right away and stop treatment if you get a rash or hives, itching, tightness of the throat, chest pain or tightness, difficulty breathing, lightheadedness, dizziness, nausea or fainting.
- Do not attempt to infuse yourself with ADVATE unless you have been taught by your HCP or hemophilia center.
What else should I know about ADVATE and Hemophilia A?
- Your body may form inhibitors to factor VIII. An inhibitor is part of the body’s normal defense system. If you form inhibitors, it may stop ADVATE from working properly. Talk with your HCP to make sure you are carefully monitored with blood tests for the development of inhibitors to factor VIII.
What are possible side effects of ADVATE?
- Side effects that have been reported with ADVATE include: cough, headache, joint swelling/aching, sore throat, fever, itching, unusual taste, dizziness, hematoma, abdominal pain, hot flashes, swelling of legs, diarrhea, chills, runny nose/congestion, nausea/vomiting, sweating, and rash. Tell your HCP about any side effects that bother you or do not go away or if your bleeding does not stop after taking ADVATE.
You are encouraged to report negative side effects of prescription drugs to the FDA. Visit www.fda.gov/medwatch, or call 1-800-FDA-1088.
For additional safety information, click here for Prescribing Information and discuss with your HCP.
*Per-Protocol: subjects who had >90% of the predicted number of infusions and no major protocol deviations.6
†44 bleeds (IQR, 20.8), 1 bleed (IQR, 4.1); IQR=Interquartile range, the range of values of the variable in a statistical distribution that lies between the upper and lower quartiles.8
References:
- Our Story. Our History. https://www.baxter.com/our-story/our-history. Accessed June 25, 2018.
- About Shire. Our story. https://www.shire.com/who-we-are/our-story. Accessed May 1, 2018.
- ADVATE Prescribing Information.
- Négrier C, Shapiro A, Berntorp E, et al. Surgical evaluation of a recombinant factor VIII prepared using a plasma/albumin-free method: efficacy and safety of Advate in previously treated patients. Thromb Haemost. 2008;100(2):217-223.
- Grillberger L, Kreil TR, Nasr S, Reiter M. Emerging trends in plasma-free manufacturing of recombinant protein therapeutics expressed in mammalian cells. Biotechnol J. 2009;4(2):186-201.
- Valentino LA, Mamonov V, Hellmann A, et al. A randomized comparison of two prophylaxis regimens and a paired comparison of on-demand and prophylaxis treatments in hemophilia A management. J Thromb Haemost. 2012;10:359-367.
- What is Prophylaxis? https://www.wfh.org/en/abd/prophylaxis/what-is-prophylaxis. Accessed June 4, 2018.
- Interquartile Range definition. MedlinePlus.
https://www.merriam-webster.com/dictionary/interquartile%20range. Accessed May 10, 2018.
© 2018 Shire US Inc., Lexington, MA 02421. All rights reserved. 1-800-828-2088.
SHIRE and the Shire Logo are registered trademarks of Shire Pharmaceutical Holdings Ireland Limited or its affiliates.
ADVATE is a trademark or registered trademark of Baxalta Incorporated, a wholly owned, indirect subsidiary of Shire plc.
S39238 07/18
 Hemophilia is a rare genetic bleeding disorder that prevents blood from clotting normally.1
Hemophilia is a rare genetic bleeding disorder that prevents blood from clotting normally.1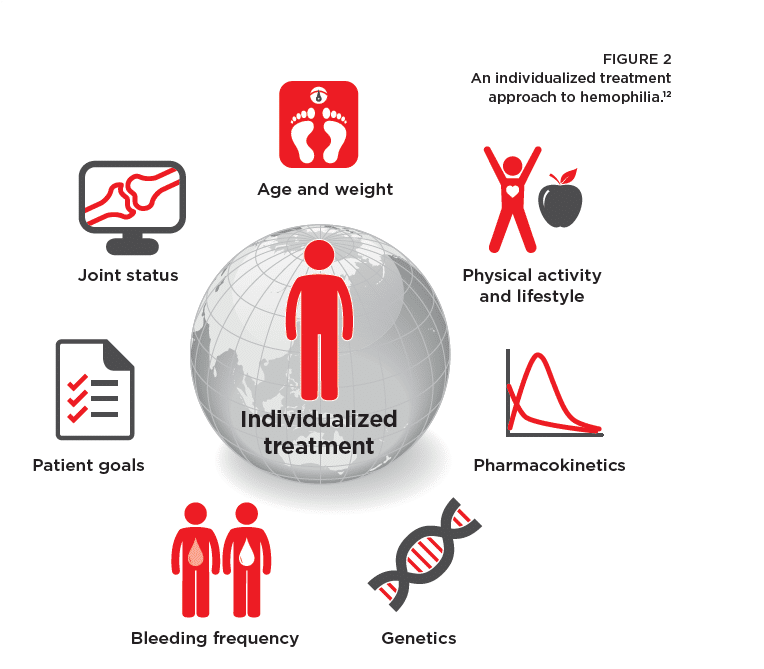 regimen to align with your unique needs and help you achieve treatment goals.
regimen to align with your unique needs and help you achieve treatment goals.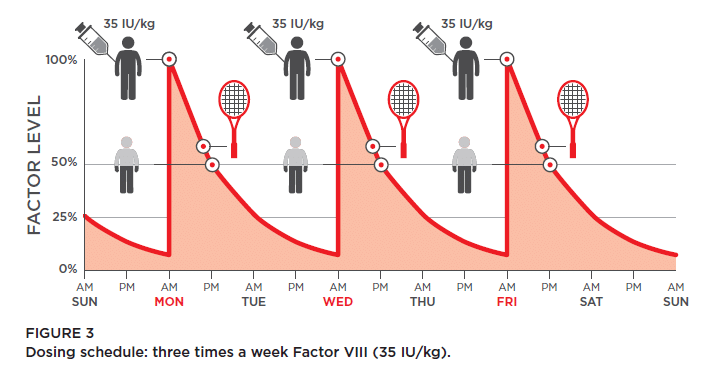

 In the years that followed, we advanced the treatment of hemophilia A, hemophilia B, hemophilia A or B with inhibitors, von Willebrand disease, and acquired hemophilia A with significant developments. Many of these were firsts: the first recombinant factor VIII treatment, the first needleless transfer device, the first recombinant factor VIII treatment free of blood-based additives, the first recombinant treatment for people with von Willebrand disease, and the first recombinant porcine factor VIII for acquired hemophilia.6-9
In the years that followed, we advanced the treatment of hemophilia A, hemophilia B, hemophilia A or B with inhibitors, von Willebrand disease, and acquired hemophilia A with significant developments. Many of these were firsts: the first recombinant factor VIII treatment, the first needleless transfer device, the first recombinant factor VIII treatment free of blood-based additives, the first recombinant treatment for people with von Willebrand disease, and the first recombinant porcine factor VIII for acquired hemophilia.6-9 Thanks to the many contributions that have been made in the past, and which Shire continues to make, to the treatment of bleeding disorders, Shire’s vision for patients with a bleeding disorder is closer to realization than ever before.
Thanks to the many contributions that have been made in the past, and which Shire continues to make, to the treatment of bleeding disorders, Shire’s vision for patients with a bleeding disorder is closer to realization than ever before. And the innovation continues. Research and development is going strong with 20 ongoing clinical trials in bleeding disorders, including one in gene therapy, as well as advancements in other novel therapies. Shire has engaged hundreds of the world’s leading scientists, researchers, and patient support specialists to help them.5
And the innovation continues. Research and development is going strong with 20 ongoing clinical trials in bleeding disorders, including one in gene therapy, as well as advancements in other novel therapies. Shire has engaged hundreds of the world’s leading scientists, researchers, and patient support specialists to help them.5 Most fundamentally, Shire is collaborating with the bleeding disorders community, including patient associations that have enabled the diagnosis of more than 30,000 hemophilia patients around the world.5 Shire has listened to, learned from, and championed their needs. This bleeding disorders community is our community. It’s why Shire is always pushing ahead, proactively shaping the future of bleeding disorders and continually elevating care for patients.
Most fundamentally, Shire is collaborating with the bleeding disorders community, including patient associations that have enabled the diagnosis of more than 30,000 hemophilia patients around the world.5 Shire has listened to, learned from, and championed their needs. This bleeding disorders community is our community. It’s why Shire is always pushing ahead, proactively shaping the future of bleeding disorders and continually elevating care for patients.

